Old screening was compliance-first
Manual checks, partial screens, paper records, subjective observations, and referral slips satisfy a file but rarely build a longitudinal child record.
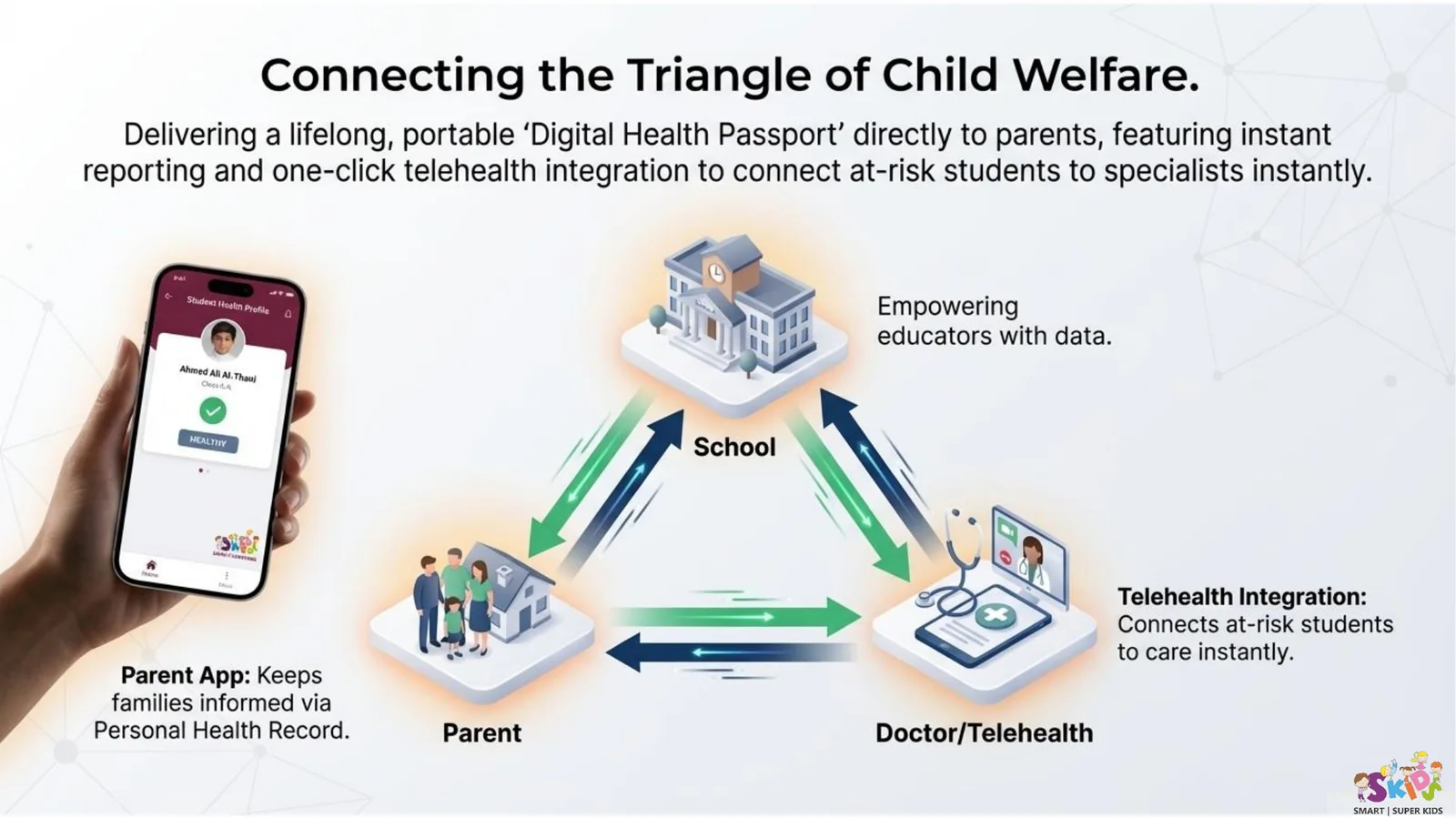
SKIDS works where children grow: home, school, community, and clinic. A SKIDS partner school runs a SKIDS School Clinic: whole-child screening, school observation, parent-readable reports, pediatrician-visible records, and a care pathway for children who would otherwise be seen only when something goes wrong.
A child who cannot see the board, hear instructions, breathe well at night, sit with comfort, or regulate attention is not simply underperforming. The body is asking for help inside the classroom.
SKIDS makes the school an extension of pediatric primary care. The principal, teachers, parents, and pediatrician are no longer holding separate fragments. The school aligns with the direction set by CBSE, WHO, UNESCO, and modern preventive-health policy, but more importantly becomes part of building the whole child.
RBSK, the School Health and Wellness Programme, WHO/UNESCO school-health guidance, and modern preventive-health priorities all point in the same direction. The weak point is execution: manual, partial, paper-based checks cannot give parents, schools, or pediatricians a full picture of the child.
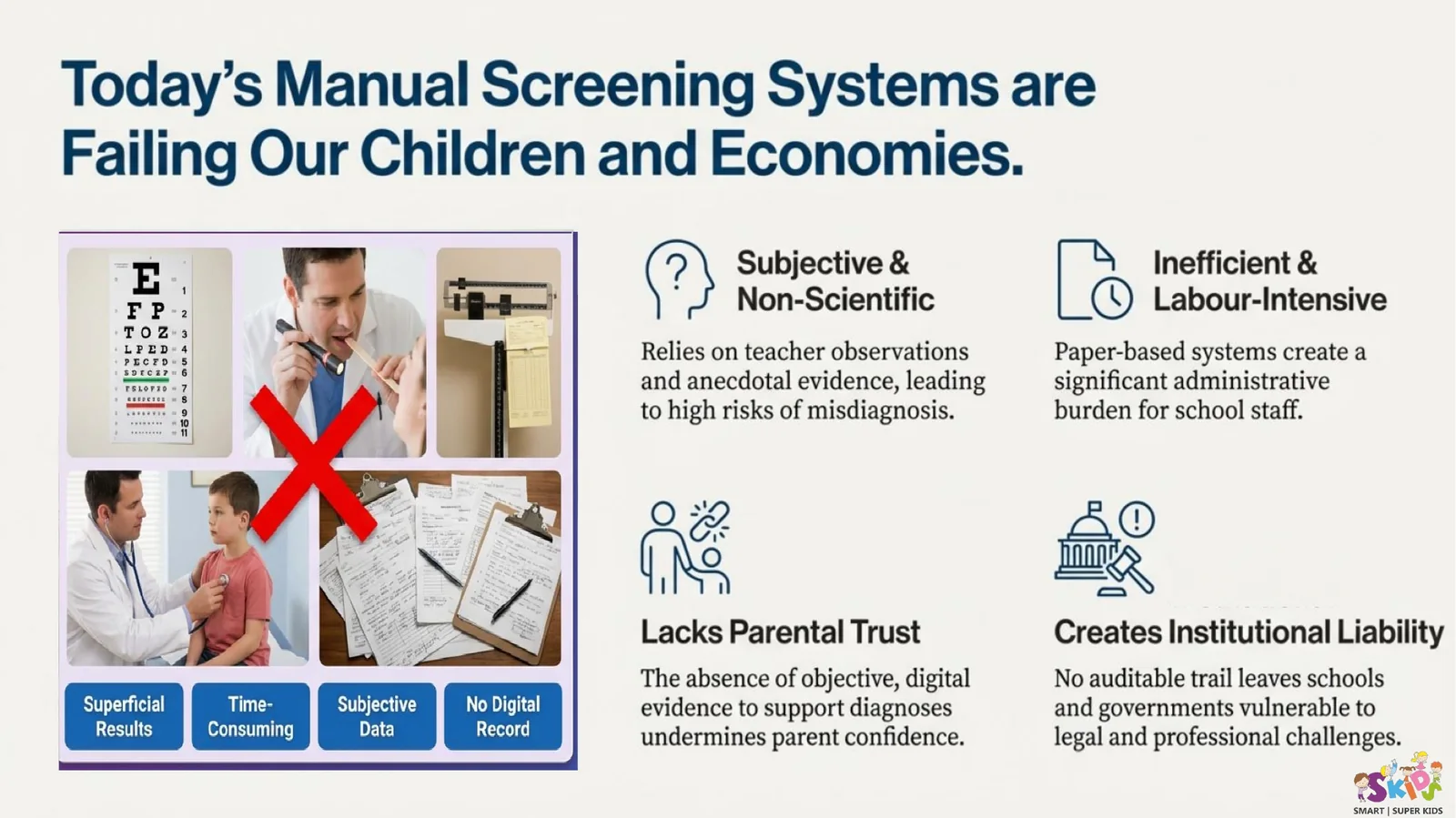
Manual checks, partial screens, paper records, subjective observations, and referral slips satisfy a file but rarely build a longitudinal child record.
Objective parameters, fast execution, auditable reports, parent-readable language, pediatric review, and a closed follow-up loop.
SKIDS becomes the school clinic operating layer: observation, devices, pediatric protocols, reports, follow-up care, and aggregate insight.
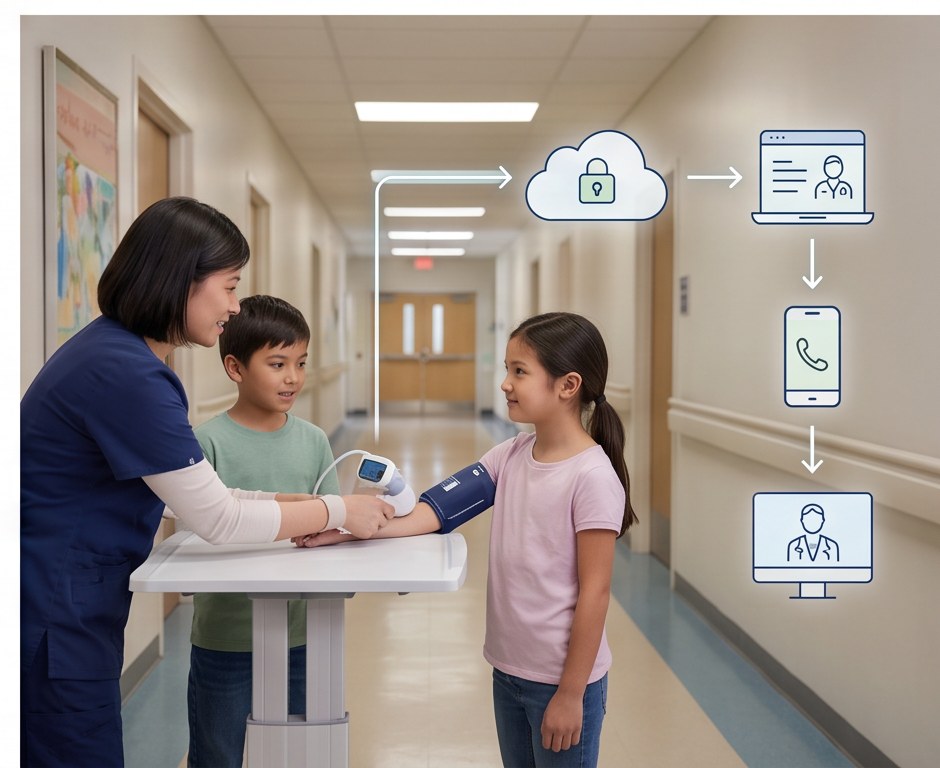
The school contributes access, context, and trust. SKIDS brings the clinical operating system: trained teams, devices, assisted signal capture, pediatric validation, parent reports, and follow-up pathways.
The school shares rosters, rooms, communication windows, and the observations teachers already hold.
Children move through calm stations for vision, hearing, growth, nutrition, oral, respiratory, and development signals.
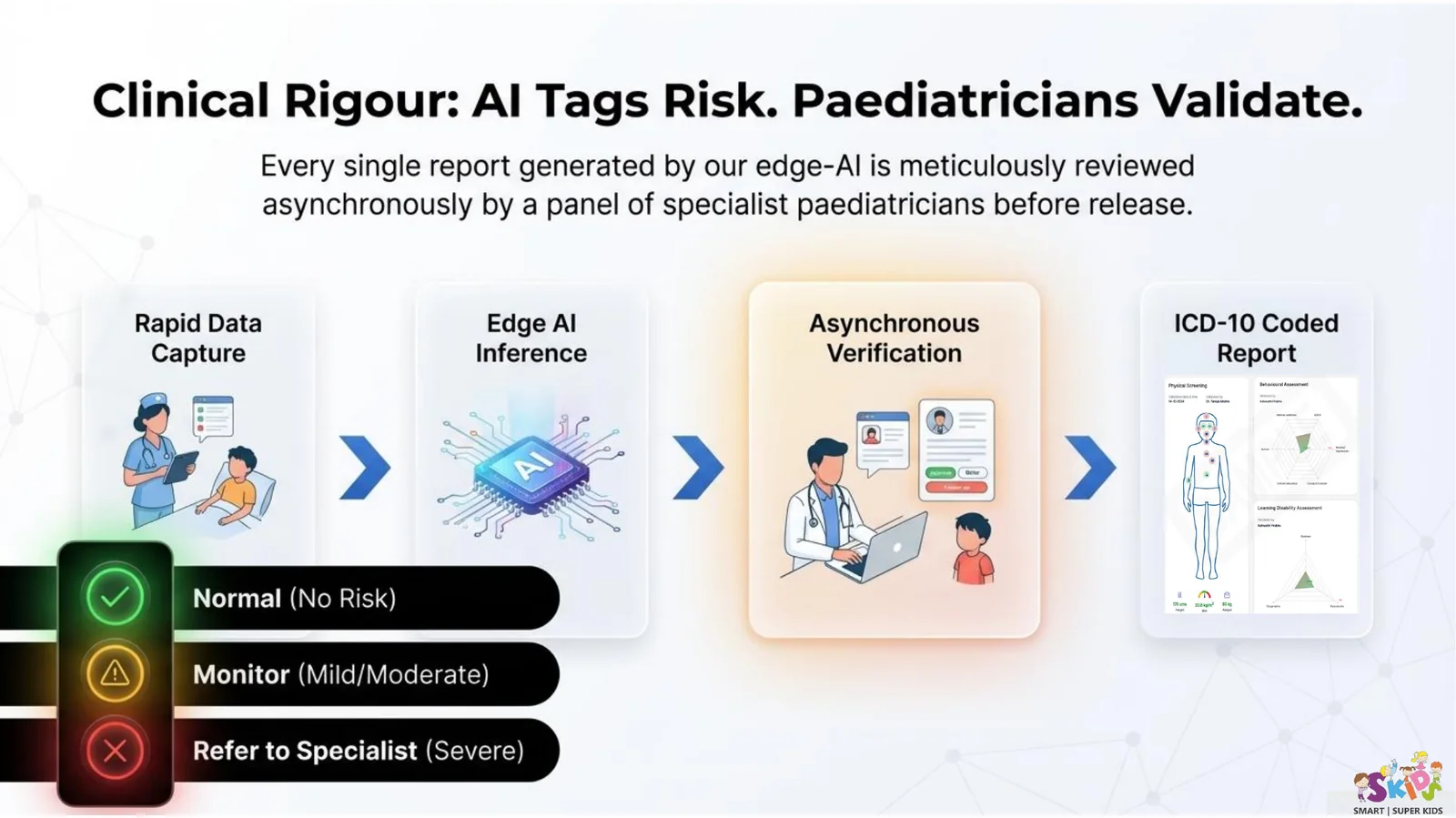
Objective signals are organised into normal, monitor, and refer pathways so the pediatric team sees what needs attention.
Findings are reviewed by the SKIDS pediatric team before they become parent-facing recommendations.
Each family receives a clear report with what was found, what it may mean, and what to do next.
At-risk children enter a care pathway, while the school sees de-identified patterns for planning and support.
SKIDS does not screen one organ and call it health. The school programme combines daily observation with whole-child screening: physical, developmental, behavioural, and learning-linked signals.
Board-copying trouble, squinting, headaches, and silent myopia risk.
Missed instructions, classroom attention, and speech-linked listening clues.
Height, weight, BMI, nutrition risk, and the pattern behind the number.
Dental signals, mouth breathing, sleep clues, and airway-linked habits.
Sleep, attention, anxiety, behaviour, and classroom participation signals.
Development, speech, learning, and school-readiness checkpoints.
The goal is not to alarm parents. It is to make the invisible visible early enough for simple, sensible care, and to give the child's pediatrician a picture that routine clinic visits rarely capture.
Children observed and screened by SKIDS school teams, with the dataset growing every year
Children with a finding worth a closer look
Parameters translated into parent-readable body signals
Parent-ready reports after the screening day


SKIDS is not limited to a camp day. The same pediatric care system can operate as a School Clinic, augment a public child-health programme, or power child-health intelligence for large systems, while keeping the same goal: better whole-child outcomes.
A school-led pediatric wellness clinic that brings whole-child screening, school observation, parent reports, pediatric review, compliance readiness, and follow-up into the life of the school.
SKIDS can augment RBSK-style and other community-oriented child-health programmes without replacing frontline teams: objective capture, faster screening, parent-ready reports, referral routing, and dashboards.
For large school-health missions, SKIDS can provide the intelligence layer: non-invasive screening, auditable digital trails, aggregate child-health indices, and dashboards for system leaders.
The exact model differs by country, but the direction is consistent: health is not a side programme. When care moves closer to the child, barriers fall earlier and schools gain a clearer view of learning readiness.
School health moved from episodic inspection into law, with schools responsible for regular medical examinations and follow-up action.
A quiet test in school became a way to find asymptomatic kidney disease before it becomes life-altering.
Health Promoting Schools made the global argument that health and learning should be planned together, not in separate silos.
The national child-health programme takes screening to children from birth to 18 years, including schools, through the 4D framework.
Ayushman Bharat's school programme, implemented with CBSE, NCERT, and UNESCO support, makes health and wellness part of school life.
Global standards for Health Promoting Schools treat school as a daily setting for living, learning, prevention, and early support.
WHO and UNESCO, Making Every School a Health-Promoting SchoolJapan's school urinary screening program shows how schools can detect silent kidney disease early, before illness becomes visible.
Kidney Research and Clinical Practice, 2024RBSK screens children for the 4Ds: defects at birth, diseases, deficiencies, and developmental delays including disability.
Press Information Bureau, Ministry of Health and Family Welfare, 2025India's School Health and Wellness Programme makes health a school responsibility, not an occasional camp.
UNESCO, CBSE and NCERT School Health and Wellness ProgrammeEconomic modelling found whole-school health models had the strongest return among school-based health promotion approaches.
European Journal of Public Health, 2021SKIDS turns a school screening day into parent-readable reports, pediatric triage, follow-up, and one life record.
SKIDS school screening operationsThe school provides access, rooms, one point of contact, parent communication support, and the observations only a school can hold. SKIDS provides staff, devices, materials, reports, follow-up, and aggregate outcomes.
Every child gets a report. Every parent gets a next step. Every school gets de-identified patterns that help leadership see what children need, without asking teachers to become doctors.
Send the school name, city, approximate student strength, your role, and one thing you would like to ask SKIDS. Response within 5 working days.